

Hormone therapy can control the progression of cancer for several years. However, over time, the cancer may start progressing again and become resistant to castration, meaning that hormone therapy no longer has the same effect. Some cells will still remain sensitive to hormone therapy, which is why it is kept as the basis.
Treatments exist to treat castration-resistant prostate cancer (CRPC), but they differ depending on the presence or absence of metastases or the rate at which your PSA rises.
At each consultation, a blood test allows your doctor to monitor your PSA level during hormone therapy. If the PSA level starts to rise, the doctor will monitor how long it takes to double. The shorter this period, the higher the risk of recurrence, and the more aggressive the recurrence will be. Prostate cancer will then have become castration-resistant.
This is a cancer that does not yet have visible metastases (diagnostic tests do not allow them to be seen), but certainly has microscopic metastases in the body that will become visible on imaging sooner or later.
In recent years, non-metastatic CRPC has been the most studied area of prostate cancer in order to find drugs capable of preventing or delaying the onset of metastases.
For patients with a rapid increase in PSA (doubling time <10 months), new generation hormone therapy may be offered. These treatments may include:
Positive results have been obtained with these three agents, showing that they all delay the appearance of metastases by about two years in patients with rapidly rising PSA (CRPC without metastases at high risk of progression).
In this situation, your doctor will describe how the treatment works and the side effects that may occur. You may also consider participating in a research protocol to benefit from new forms of therapies.
When prostate cancer is resistant to standard hormone therapy and there is evidence of metastases on examination, treatment must be initiated. This treatment will depend on several factors including age, comorbidities, the presence of symptoms secondary to cancer, and the rate at which cancer develops.
For over 10 years, several studies have allowed the approval of multiple treatments for patients at this stage. However, these treatments do not cure cancer. Even with the use of these treatments, standard hormone therapy must continue to be taken.
1- Docetaxel (chemotherapy): The first treatment to be approved in this area, it provides rapid relief of symptoms secondary to cancer. It is usually administered every 3 weeks by intravenous infusion at the hospital.
2- Abiraterone (hormone therapy): This is a daily medication that allows for greater hormonal castration. Regular blood tests are necessary.
3- Enzalutamide (hormone therapy): This is a daily medication that allows for greater hormonal castration.
4- Radium-223 dichloride (radiopharmaceutical): This is a radiological treatment by weekly intravenous infusion for six weeks. The medication circulates in the blood and attaches to bone metastases emitting radiation. It is usually reserved for patients with bone metastases only.
5- Cabazitaxel (chemotherapy): This is a chemotherapy usually reserved after failure of docetaxel.
6- Lynparza (iPARP): This is a PARP inhibitor that prevents cancer cells from repairing damage to their DNA, eventually leading to the death of these cells. See our animated capsule for more understanding on this protein family called PARP.
7- Pluvicto (radiopharmaceutical medication): This is a medication that delivers radioactive treatment directly to the cancer cells to be treated. This type of therapy is sometimes the best option for treating metastatic prostate cancer that no longer responds to other treatments. See our animated capsule for more understanding on this type of treatment.
8- Sipuleucel-T: This is a vaccine made from the patient’s white blood cells. Sipuleucel-T is a therapeutic vaccine, intended to treat metastatic prostate cancer, not to prevent it. It is extremely expensive and is not currently offered in Canada.
Understanding the hereditary and genetic aspects of this disease can provide valuable information to both individuals affected and their families.
Are you over 50 or experiencing urinary problems? Discover why early screening for prostate diseases is important.
Do you have a family history of cancer? Your doctor might recommend genetic screening.
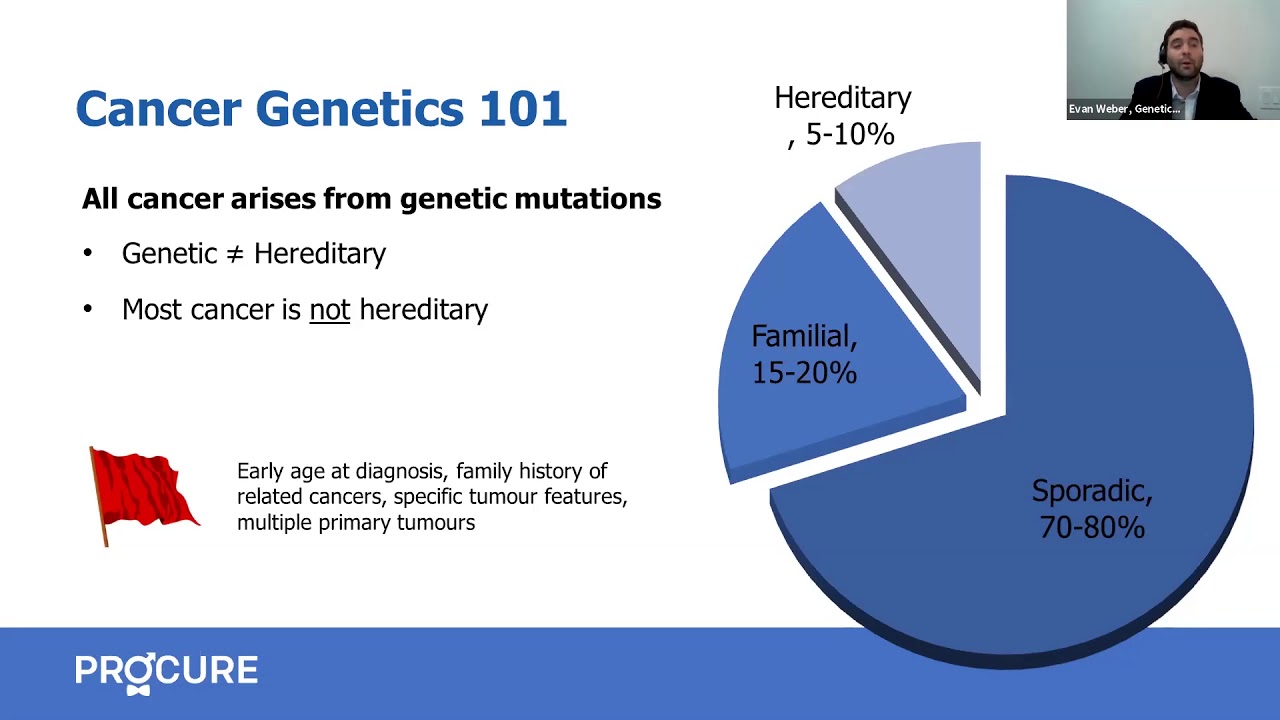
Although rare, some hereditary genetic mutations can increase your risk of prostate cancer.
Learn about the role of your prostate, related diseases, symptoms to watch out for and risk factors.

The Benefits of Vitamin D A great amount of research present the multiple benefits of Vitamin D. For example, Vitamin D regulates the amount of calcium and phosphorus, helps build bones and brings many more benefits to other tissues in the body, including kidneys, intestines and parathyroid glands. In fact, past reasearch found a link […]

The exact causes of prostate cancer are not yet well understood. Researchers have found some risk factors and are trying to determine how these factors lead to prostate cancer.

Being overweight or obese may increase a man’s risk of aggressive prostate cancer, researchers believe after doing animal and human cell studies.
Sources and references
Last medical and editorial review: April 2024. See our web page validation committee and our collaborators by clicking here.