


Strategies for treating advanced cancer have significantly evolved, offering new options and hope for patients.
Summary of clinical trial results on promising prostate cancer research.
Clinical trial results on triple therapy for advanced hormone-sensitive prostate cancer.
What you need to know about hormone therapy and how to manage the side effects of this treatment.
What about nuclear medicine? Is it suitable for your situation?
Has your doctor suggested prostate imaging tests? Explore options like PSMA PET scans.
If you have a specific genetic mutation, you could benefit from new targeted treatments.
Do your recent tests show an increase in PSA levels? It could indicate a recurrence.
Has your doctor recommended hormone therapy? This video is for you!
Strategies for treating advanced cancer have significantly evolved, offering new options and hope for patients.
Advanced prostate cancer encompasses various conditions, including metastatic, recurrent, and hormone-resistant forms, each raising different questions and concerns.
A recurrence is when the cancer returns after treatment. The main question is, “What’s next?”
Advanced prostate cancer encompasses various conditions, including metastatic, recurrent, and hormone-resistant forms, each raising different questions and concerns.
Hormone therapy can reduce tumor size, control cancer, and prolong life. Is it the right treatment for your cancer?
In this interview, we answer patients’ questions about new therapies for advanced prostate cancer.

Find out if you are eligible for radioligand therapy for prostate cancer, how the treatment works, and the precautions to follow.

Learn how radioligand therapy helps slow advanced prostate cancer and why access to this treatment varies across Canada.
Discover how biomarkers personalize and guide prostate cancer treatment decisions for each patient.

Learn how biomarkers enable more precise monitoring and treatment of prostate cancer.
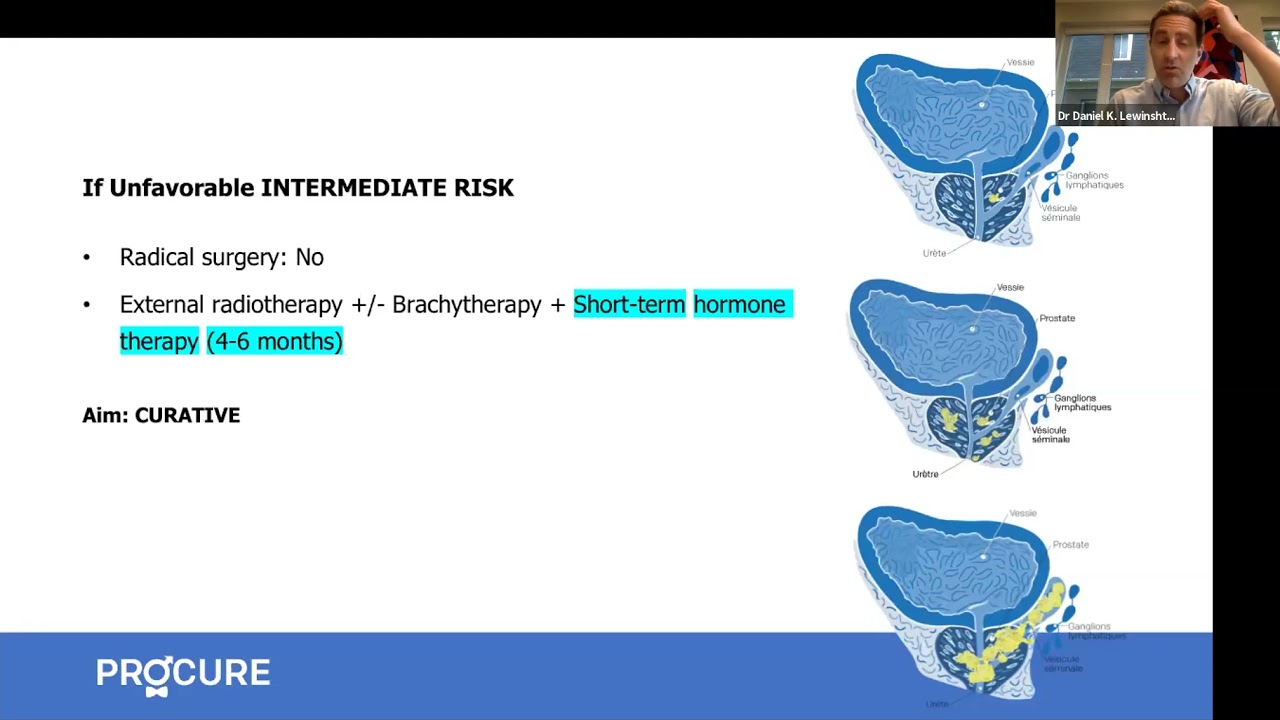
Discover the available treatments, new targeted therapies, and the next steps in managing a prostate cancer recurrence.

Learn how hormone therapy and PARP inhibitors work in your body and what side effects to anticipate.

When prostate cancer progresses to an advanced stage, it can spread to the bones. This is where a bone scan plays a role.
Understand the purpose of your tests (PSA, MRI, PSMA PET scan, biopsy, bone scan) to better navigate them.

Which approach is better: continuous or intermittent hormone therapy?